
X
Trustworthy Source
PubMed Central
Journal archive from the U.S. National Institutes of Health
Go to source
A CIDP diagnosis is based on clinical symptoms, electrodiagnostic studies, and additional laboratory tests. CIDP can only be diagnosed by a medical professional. By recognizing the symptoms of CIDP, seeking a medical diagnosis, and learning about the condition, you can better collaborate with your doctor to diagnose CIDP.
Recognizing Symptoms of CIDP

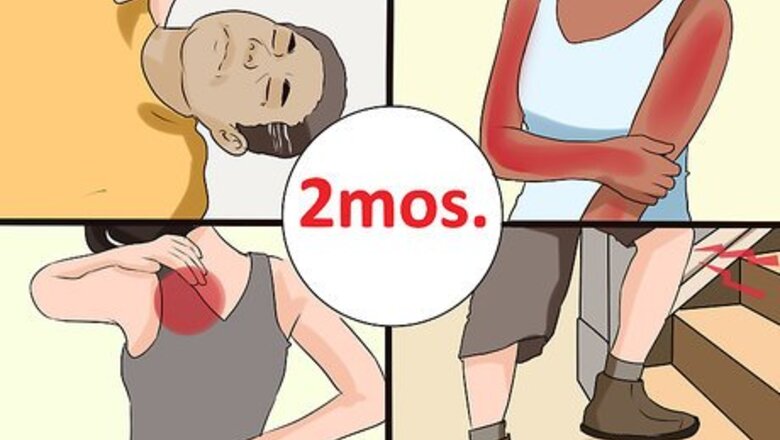
Experience primary physical symptoms. CIDP is closely related to Guillain Barré syndrome (GBS), and many of the symptoms are similar. The first signs that a person may have CIDP include "motor deficiencies," like physical weakness and pain. These symptoms usually progress slowly over a period of two months. It is important to note that these symptoms could indicate a wide-variety of treatable conditions, and do not alone indicate CIDP. Some of these physical symptoms may include: Weakness Numbness Difficulty walking (especially on stairs) Tingling Pain Fainting spells (while standing up) Burning in the extremities Sudden onset of back and/or neck pain that radiates through the limbs

Recognize autonomic dysfunction. Other signs of CIDP fall under the category of “autonomic dysfunction.” These "sensory" symptoms may appear after the onset of primary physical symptoms. They may also progress over a period of weeks. Once again, these symptoms could indicate any number of treatable conditions, and do not alone point to CIDP. Symptoms include: Dizziness Difficulty breathing Bowel and bladder problems Nausea Eye twitching (ranging from mild to severe) Twitching or shaking in other parts of the body

Keep track of your symptoms. Symptoms of CIDP usually progress over an 8-week period, gaining intensity. This slow (either steady or step-wise) development of symptoms over an 8-week period is one of the best ways to distinguish this disorder from the more common Guillain Barré syndrome (GBS). As such, it is very important to have a record of when symptoms began, and how they have progressed. Start a health journal. Write down a quick note about how you feel each day. Include dates for when symptoms began. Include a note about the severity of symptoms.

Consider your age. CIDP has been detected in people of all ages (including children). However, people between the ages of 50 and 60 are far more likely to be diagnosed. Take your age into consideration when attempting to diagnose CIDP.
Getting a Medical Diagnosis

Speak to your doctor. If you are experiencing any of the above symptoms, make an appointment to speak with your doctor. Your doctor may want to refer you to a neurologist or other specialist. At your appointment, be ready to explain: Any symptoms. Keep in mind that symptoms will follow one of three patterns including progressive (symptoms get worse over time), recurrent (symptoms come and go in episodes), and monophasic (symptoms last for one to three years and don’t recur). When your symptoms began Your medical history Any other conditions you have Any medications you are taking

Undergo a physical examination. When your doctor evaluates you for CIDP, they will begin by performing a physical examination. They will track your weight, temperature, and blood pressure. They will test the strength of your muscles and tendons, as well as your balance.

Prepare for “electrodiagnostics” tests. Next, your doctor will look for myelin damage in peripheral nerves. This can be done by way of an electromyography test (EMG) and/or nerve conductive study (NCS). These tests are non-invasive, but they can be uncomfortable. They involve using gentle electrical currents to test nerve function and response. These tests will be looking for nerve damage, or “demyelination.” This can be indicated by: Reduction in nerve velocities A conduction block in one or more nerves The presence of abnormal temporal dispersion in one or more nerves Prolonged distal latencies in two or more nerves

Run blood and urine tests. In order to rule out other conditions—such as diabetes, infections, toxin exposure, nutritional deficiencies, inflammatory disease of blood vessels, and/or other autoimmune diseases--your doctor will run tests on both your blood and urine.

Experience a “lumbar puncture.” A lumbar puncture will look for anti-ganglioside antibodies. Although these antibodies may not be present in all cases of CIDP, there is a branch of CIDP diseases characterized by anti-GM1, anti-GD1a, and anti-GQ1b. A lumbar puncture involves the insertion of a small needle into the back where cerebrospinal fluid (CSF) is drawn. This fluid is then tested for the presence of these antibodies.

Undergo a sural nerve biopsy. In rare instances where the diagnosis is not clear, or where other causes of neuropathy cannot be excluded, your doctor may request a biopsy. This outpatient procedure involves a 4–5 centimeter (1.6–2.0 in) incision in the leg (with the aid of local anesthetic). Through the incision, a 1–2 centimeter (0.39–0.79 in) piece of the sural nerve is excised, and then studied. This procedure is done while you are under anesthesia.
Learning About CIDP

Start with typical CIDP. CIDP is rare autoimmune condition that causes the body to fight against its own tissues. CIDP causes the body to attack the myelin sheaths that protect nerves, ultimately leading to nerve damage. CIDP often manifests as motor and sensory dysfunction. Motor deficits (such as weakness, difficulty walking) are reported in 94% of CIDP patients. Sensory deficits (such as numbness, poor balance) are reported in 89% of CIDP patients.

Learn about sensory/motor predominant CIDP. In 5-35% of CIDP patients, sensory symptoms will occur predominantly, with little to no motor deficits. On the opposite side, 7-10% of CIDP patients (more often patients under the age of 20) experience motor-related symptoms, with little to no sensory deficits.

Explore Lewis-Sumner syndrome (LSS). Lewis-Sumner syndrome (LSS)--also known as multifocal acquired demyelinating sensory and motor neuropathy (MADSAM)—presents in 6-15% of CIDP patients. This form of CIDP is characterized by asymmetry, where symptoms affect one part of the body (usually the upper body/upper limbs) more than others.

Research CIDP treatments. Although the exact cause of CIDP is still unknown, this condition is treatable. Particularly when the condition is diagnosed early on, many patients experience remission and recovery from symptoms without long-term nerve damage. Your treatment plan will be based on the specific brand of CIDP you are experiencing, your symptoms, and any other conditions you may have. Some forms of CIDP treatment include: Corticosteroids, such as prednisone Immunosuppressant drugs Plasmapheresis (plasma exchange) Intravenous immunoglobulin (IVIg) therapy Physiotherapy

















Comments
0 comment